DISCLAIMER: THIS WEBSITE DOES NOT PROVIDE OPTICAL ADVICE
The information, including but not limited to, text, graphics, images and other material contained on this website are for informational purposes only. The purpose of this website is to promote broad consumer understanding and knowledge of eyecare. It is not intended to be a substitute for professional optical advice, diagnosis or treatment. Always seek the advice of your optician
or other qualified eye care providers with any questions you may have regarding a medical condition or treatment, and before undertaking a eye test, and never disregard professional medical advice or delay in seeking it because of something you have read on this website.
How the Human Eye works
The diagram to the right shows the key parts of the human eye.
Imagine the eyeball as a small, hollow ball, measuring approximately 2cm from front to back. The only way that light can enter the eye is through the pupil, a small circular opening in the centre of the iris at the front of the eye. When you look at someone’s eye, the pupil is the small black disc at the centre of the coloured part of the eye, the iris. Tiny muscles in the iris will contract and relax to allow the pupil to change in size and therefore control how much light can enter the eye. On a bright, sunny day you will notice that the pupil is quite small, whilst at night the eye needs as much light as it can get and therefore the pupil is large. In older people the pupil naturally decreases in size and shows less variation in size.
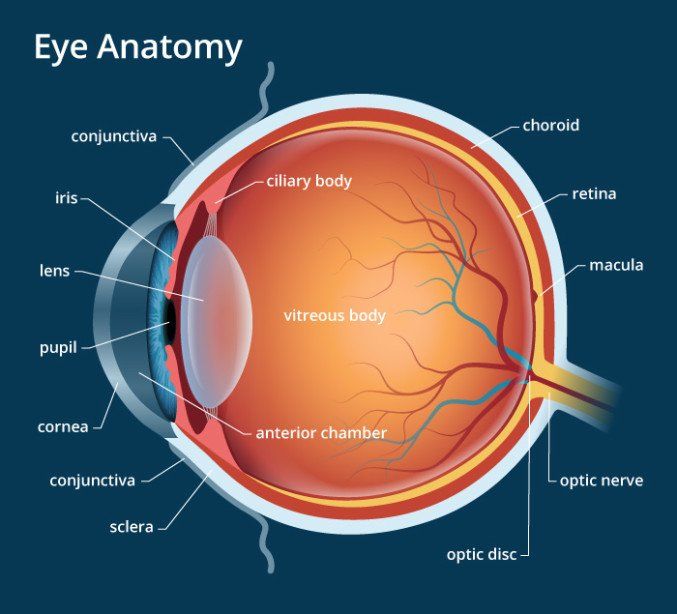
The inner lining of the tough wall of the eye is the retina, a very thin, light-sensitive membrane. The main cavity inside the eye
is filled with a clear jelly-like substance called the vitreous, which for much of your life is pushed up against the retina.
As light rays enter the eye, they must be focused to form an image on the retina. The focusing is done by the cornea and the lens.
The lens can change its focusing power by changing shape. This is controlled by a small ring of muscle around the lens.
Unfortunately, as we go through life the lens becomes less flexible and so cannot alter its focus. This is why we all develop
problems with focusing on objects at different distances and why so many of us require reading glasses in later life.
Six tiny muscles around each eye control the position of the eye and ensure that when you look directly at an object, the
image of that object falls onto the special part of the central retina called the fovea or macula. Light falling onto the retina
stimulates millions of tiny nerve cells. All of these tiny retinal nerves come together at the back of the eye to form the optic
nerve, which carries the image information along to the visual cortex at the back of the brain, allowing you to ‘see’ the image.
Age Related Macular Degeneration
What is Age Related Macular Degeneration (AMD)?
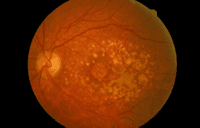
The macula is the central part of the light-sensitive retina at the back of the eye (see ‘How the Eye Works’). When you look directly at an object, you are using the macula to discern the fine detail. The macula also allows you to see colour.
Unfortunately as we go through life the macula is particularly susceptible to age related degenerative changes and these can cause the delicate cells of the macula to stop working. People with AMD therefore have particular problems seeing detail such as writing but because the rest of the retina still works normally they are able to see objects around them.
Unfortunately as we go through life the macula is particularly susceptible to age related degenerative changes and these can cause the delicate cells of the macula to stop working. People with AMD therefore have particular problems seeing detail such as writing but because the rest of the retina still works normally they are able to see objects around them.
There are principally two types of AMD know as ‘wet’ and ‘dry’. The majority of AMD is of the dry type.
In dry AMD the cells of the macula are damaged over a long period of time and people tend to experience a gradual loss of central vision.
In wet AMD, as the cells of the macula degenerate they allow new small blood vessels to grow underneath the retina. These new blood vessels are very delicate and are prone to leak or rupture. This allows blood or fluid to collect under the macula and this can cause a rapid and severe decline in central vision. People with ‘wet’ AMD usually start with signs of only ‘dry’ AMD but as the disease progresses signs of ‘wet’ AMD develop.
AMD usually affects both eyes, although one eye may be affected long before the other.
What causes AMD?
Although there is a great deal of research into AMD going on around the world, the exact cause of AMD is still unknown but the following factors are known to be important:
Age – unfortunately as the name suggests, growing older makes AMD much more likely.
Gender – women seem more likely to develop AMD than men.
Genetics - your genes appear to have some influence on whether you develop AMD but at the moment this is not fully understood.
Smoking – smoking has been linked to the development of AMD. Studies have also shown that stopping smoking can help to prevent AMD
Sunlight – some research suggests that long-term exposure to sunlight may affect the retina. It is a good idea to wear sunglasses.
Nutrition – research suggests that some minerals and vitamins can help to protect against AMD.
Can I prevent AMD?
Clearly there is nothing you can do about your age, gender or genetics. However, stopping smoking, protecting your eyes from the sun by wearing sunglasses and eating a balanced diet with plenty of dark green vegetables are all useful steps to take. Some people take specific dietary supplements in the form of tablets to help prevent AMD but current research suggests that these are only really indicated for people already showing signs of AMD.
You cannot ‘wear out’ your eyes by reading or watching television, even if your vision is already affected by AMD.
How would I know if I have AMD?
Most people with dry AMD simply become aware that they are struggling more to see detail such as small print although sometimes people see a dark, blurred or blank spot in their central vision. When wet AMD is developing, people often notice that straight lines, such as door frames and windows, look wavy or distorted. This will often come on quickly, perhaps over a few hours or overnight.
Your optometrist, when carrying out a routine eye examination, will be able to see signs of AMD at the back of your eye. If you are concerned that you may be developing AMD, make an appointment to see your optometrist. If you feel that your vision has changed quickly or you are aware of distorted vision as described above, please seek prompt attention with your optometrist or an eye doctor.
Is there any treatment for AMD?
There is currently no treatment for dry AMD.
Over the years various treatments for wet AMD have come and gone with very limited success but the latest of these has been shown to be a significant breakthrough and effective in halting the progression of vision loss. The newest treatment involves a series of injections into the eye (apparently not as awful as it sounds) over a period of months or years. This treatment is now available on the NHS at specialist centres but must be administered in the early stages of the disease. If you think you may have wet AMD (distorted or quickly reducing vision in one eye) please seek attention promptly.
More useful information about AMD can be found at the following websites:
Cataract
Cataract occurs when the lens inside the eye becomes cloudy (see ‘How the human eye works’) causing vision to become misty or blurred. It is not a skin growing over your eye, despite what you may have heard.
Most cataract is ‘age related cataract’. As we go through life our lenses naturally lose some clarity and so cataract is very common in people over the age of 60. Early cataracts do not affect your vision and do not require treatment.

Sometimes babies are born with (‘congenital’) cataract in one or both eyes. This is due to factors affecting the baby during its development. The information in this article relates to age related cataract. To find out more about congenital cataract you can visit the RNIB website at the end of this article.
How would I know if I had a cataract?
Cataracts are not painful but can affect your vision in several ways.
People with cataract often notice that their vision seems misty or blurred and perhaps get the feeling that they need to clean their glasses. Although cataracts tend to affect both eyes, one eye is usually more affected than the other, so you may only notice these symptoms in one eye. People often notice that it is hard to recognise people’s faces when you see them down the road or that the golf ball disappears against the sky.
Drivers with cataract are usually more troubled by the glare of oncoming headlights or the sun when it is low in the sky.
What causes cataract?
The transparency of the lens in the eye is due to the very regular arrangement of the cells that make up the lens. As we go through life this arrangement is gradually disturbed causing the lens to become cloudy. In this sense, everyone will eventually develop cataract to some degree and so age is the biggest risk factor in cataract. However, some people develop cataract at an earlier age than others. This may be partly hereditary but other factors such as exposure to ultraviolet light, smoking, eye injuries and other diseases or medication are important.
Can cataracts be prevented?
We can’t help getting older but we can reduce the risk of cataract by:
Not smoking! Oxidising agents in cigarettes are known to accelerate the process of cataract.
Protect your eyes from the sun. This is particularly important for children as their eyes are more susceptible to the effects of sunlight. It has been estimated that by the age of twenty an individual will have received 80% of their lifetime exposure to ultraviolet light. So wear good UV absorbing sunglasses to protect your eyes.
Can cataracts be treated?
Treatment of cataract requires surgery to remove the cloudy lens from the eye. Cataract cannot be treated by ‘laser.’ In recent years the techniques of cataract surgery have improved dramatically. The surgery is usually performed under local anaesthesia to help the patient recover more quickly and avoid the need to stay overnight in hospital. Using a special instrument the surgeon breaks up the cataract into tiny pieces which can then be easily removed from the eye before a new plastic lens is inserted into the eye to replace the old lens and help the eye to focus.
More useful information about cataract can be found at the following websites:
Glaucoma
What is glaucoma?
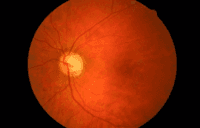
Glaucoma is the name for a group of eye conditions which cause damage to the optic nerve at the back of the eye. When the optic nerve is damaged the visual information from your eyes cannot reach the brain (see how the human eye works), resulting in permanent sight loss.
People often talk about pressure in the eye when they discuss glaucoma, but glaucoma is not just about eye pressure. All eyes need a certain amount of pressure inside them to maintain the shape of the eye. In some types of glaucoma the pressure becomes abnormally high and it is thought that this pressure directly damages the optic nerve. However, in other types of glaucoma, the eye pressure is normal and it is thought that a weakness in the optic nerve leads to damage and visual loss.
People often talk about pressure in the eye when they discuss glaucoma, but glaucoma is not just about eye pressure. All eyes need a certain amount of pressure inside them to maintain the shape of the eye. In some types of glaucoma the pressure becomes abnormally high and it is thought that this pressure directly damages the optic nerve. However, in other types of glaucoma, the eye pressure is normal and it is thought that a weakness in the optic nerve leads to damage and visual loss.
Would I know if I had glaucoma?
In a small number of cases, glaucoma is associated with very high levels of eye pressure. Extreme eye pressure produces significant pain and redness of the eye. People often feel sick with the pain and report seeing haloes around lights at night. This type of glaucoma is a medical emergency and requires immediate treatment to reduce the eye pressure.
Sometimes people will have episodes of raised eye pressure before a full blown attack and so it is important not to ignore symptoms of pain and redness in one eye, particularly if associated with haloes around lights.
Most glaucoma however is not associated with very high eye pressure and therefore has no symptoms in the early stages of the disease.
How can glaucoma be detected?
Whenever you have an eye examination, the optometrist is always looking for signs of glaucoma. Having regular eye examinations should mean that glaucoma can be detected at an early stage before significant optic nerve damage has occurred.
•
Measuring your level of vision
• Measuring the eye pressure
• Examining the optic nerve for signs of glaucoma damage
• Examining the eye for signs that may predispose you to developing glaucoma
• Measuring the visual field for signs of early vision loss
• Optic nerve head photography to help detect subtle changes over time
• Measuring corneal thickness as thin corneas are associated with higher risk of glaucoma
The optometrist will look at the results of these tests and consider any other predisposing factors such as family history to judge whether you may be developing glaucoma.
Your GP will not be able to tell you if you have glaucoma.
Can glaucoma be cured?
Glaucoma cannot be cured but it can be treated in an attempt to minimise the effect on vision. Glaucoma is usually treated by using eyedrops once or twice per day and this treatment must be continued indefinitely. In some cases glaucoma is treated by laser or surgery.
For glaucoma to be successfully treated it is important that it is diagnosed at an early stage before significant loss of sight has occurred.
More useful information about glaucoma can be found at the following websites:
Low Visual Aids
We offer a wide range of magnifiers and visual aids designed to help those with any visual impairment.
We are able to demonstrate many of these aids to patients, following a visual assessment, to find the most suitable device for each individual.
We are able to demonstrate many of these aids to patients, following a visual assessment, to find the most suitable device for each individual.